Journal of Addiction and Addictive Disorders
Scott Giacomuccia*; Sharon Gerab; Darrell Briggsc; & Kim Bassd
abcdMirmont Treatment Center, Lima, PA, USA
*Contact Scott Giacomucci at Scott@SGiacomucci.com for any correspondence related to this article.
aScott Giacomucci is Director of Experiential Trauma Services at Mirmont Treatment Center and founder of the Phoenix Center for Experiential Trauma Therapy in West Chester, PA.
bSharon Gera is a Behavioral Health Therapist and Certified EMDR practitioner at Mirmont Treatment Center’s inpatient unit.
c Darrell Briggs is a Behavioral Health Therapist and facilitator of services for emergency responders at Mirmont Treatment Center’s inpatient unit.
d Kim Bass is a Behavioral Health Therapist at Mirmont Treatment Center’s outpatient unit.
Experiential Addiction Treatment: Creating Positive Connection through Sociometry and Therapeutic Spiral Model Safety Structures
Abstract
Many argue that addiction is preceded by a sense of psychosocial dislocation, experiences of relational trauma, attachment ruptures, or neglect. The lived experience of drug addiction is incredibly isolating and likely to disrupt relationships with one’s closest attachment figures. Most agree that one’s social experiences – relationships, family, groups, and community – significantly impact the chances of recovery after addiction. Sociometry, the study of groups and interpersonal dynamics within groups, is uniquely effective in providing clients with corrective relational experiences in addiction treatment groups. This article outlines multiple experiential sociometry tools that hold the potential to cultivate safety, explore similarities between group members, establish group cohesion, and assess the group based on chosen criteria. These action-based sociometric processes, in addition to two safety structures from the Therapeutic Spiral Model (TSM) of psychodrama, are outlined with clinical vignettes depicting their utilization at Mirmont Treatment Center. These strength-based group structures can be adapted with different criteria, different populations, and used in any type of group setting.
Keywords: Addiction; Trauma; Sociometry; Therapeutic Spiral Model; Isolation; Group Therapy
Introduction
Addiction is a complex mental health issue influenced by multiple factors, including (epi)genetics, trauma, loss, alienation, consumerism, and multiple societal forces (Alexander, 2008; Maté, 2010; SAMSHA, 2017). An addiction treatment center is uniquely positioned to target the factors of clients’ experiences, relational trauma, loss, and isolation. The social nature of a treatment center’s community provides a response to the isolation that so often characterizes substance use disorder.
Many have highlighted isolation is one of the primary causes or underlying factors of drug addiction (Alexander, 2008; Jellinek, 1952; Maté, 2010). Alexander (2008) argues that addiction is an adaptation to social dislocation – “It is a functional way of responding to and dealing with dislocation. It is even a creative response that, for a while, can reduce the pain of dislocation.” Recent neuroscience research has shown that physical and social pain look identical in the brain (Eisenberger, 2012) – which supports what drug users already know – opiates (and other drugs) work to reduce both types of pain (Panksepp et al., 1978)! From an evolutionary perspective, separation from the social group meant certain death – “this is why forced dislocation, in the form of ostracism, excommunication, exile, and solitary confinement, has been a dreaded punishment from ancient times until the present” (Alexander, 2008). From birth, human beings are dependent on relationships with their caregivers longer than any other living creature (Cozolino, 2014). As an individual progresses through the stages of psychosocial development, she is sorting out her place in society and develops an interdependence within multiple subgroups of society (family, neighborhood, classroom, sports team, workplace, etc.) (Erikson, 1963; Alexander, 2008). This interdependence between individual, subgroups, and society has been called psychosocial integration (Alexander, 2008). In healthy development, psychosocial integration lends itself to a sense of belonging, community, and individual identity or ego strength.
Relationships are crucial to our ability to regulate our emotions that throughout our lifespan, especially in the face of threat or danger (Porges, 2017). Social connection, relationships, and community are significant components in addiction treatment and recovery (Alexander, 2008; Maté, 2010; McGregor & Bowen, 2012). The emphasis of most addiction treatment programs and recovery approaches includes significant dyadic relationships (therapist, sponsor, mentor, etc), regular small group participation (group therapy, 12-step meetings, recovery house, fellowship meetings, etc), and membership of a larger community (12-step fellowship, organized religion, spiritual group, recovery movement, etc). Alexander’s seminal “Rat Park” research highlights just this – that the presence of relationships and community was the most important variable impacting rat’s choice of drug use (2010). Many have even gone as far as to offer a conceptualization of addiction as an attachment disorder (Flores, 2011). In this light, it is especially important for addiction professionals to consider looking to the practice of sociometry to inform treatment interventions and program structures.
Sociometry and Safety Structures
Sociometry is the study of sociodynamics – or patterns of relationships within an identified group (Hale, 1981). Sociometry, developed in the early 1900s within the context of J.L. Moreno’s triadic system of sociometry, psychodrama, and group psychotherapy (Moreno, 1953), which offers addiction professionals a series of experiential group tools for assessing, strengthening, and enriching the relationships within a group. Sociometric processes can be completed on paper or in action to explore group dynamics (Moreno, 1937). While sociometry focuses on the interpersonal relations of a group, psychodrama explores, enacts, and externalizes the intrapsychic reality of an individual. Psychodrama is an experiential form of therapy (though it is also used in non-clinical settings) that involves role-playing and various other techniques (Dayton, 2005). While much has been written about psychodrama elsewhere, sociometry has not been given the same attention.
In addition to classical sociometry, the Therapeutic Spiral Model (TSM) developed with an emphasis on safety, containment, and strengths for working with trauma (Giacomucci, in-press; Hudgins, 2017). TSM offers six safety structures which are sociometric in nature and incredibly restorative for addictions group work (Hudgins & Toscani, 2013). The six safety structures are: Observing Egos, Circle of Strengths, Spectrograms, Hands-on-Shoulder Sociograms, Step-in Sociometry, and an art project. These safety structures, with the exception of the art project, will be highlighted below with an emphasis on their capacity to form group cohesion. TSM also offers its clinical map to guide the selection and implementation of sociometric criteria while facilitating these processes. The clinical map instructs one to begin with safety and strength-based criteria, then move into criteria based on defenses, trauma, and addiction, and to finish with transformative-based criteria to cultivate integration, meaning-making, and post-traumatic growth (Hudgins, 2017). TSM’s three-stage clinical map is highly compatible with other three stage models in trauma theory (Coutouis & Ford, 2015; Herman, 2015)
Sociometry tools have been used in addiction treatment for several decades and seem to be growing in popularity (Dayton, 2005, 2014, 2015; Fuhlrodt, 1990; Giacomucci, 2017; Hale, 2009; Hudgins & Toscani, 2013; Tierney, 1945). Mirmont Treatment Center is one such facility that has developed robust clinical programming which incorporates a variety of experiential sociometry-based groups. The following sections outline the use of sociometry and TSM safety structures in Mirmont’s inpatient program. It is important to note that these experiential processes can be adapted for use in any group setting (including in education, trainings, supervision, community groups, and treatment groups) with any topic.
Observing Ego Cards and Dyads
The Observing Ego (OE) is a neutral observing role. It is the first psychological function necessary for change (Hudgins & Toscani, 2013). Practicing this role in the sub-groups contributes to mindfulness practices, which are a significant part of many addiction treatment approaches (Lawrence, 2015). Developing non-judgmental awareness skills from a strength perspective appears to be impactful for people who struggle with the devastating consequences of addiction. One way the OE is portrayed is with TSM-designed Animal Cards. The cards contain an animal’s picture and strength word. Choosing a specific card helps concretize and externalize the internal part of self that can observe the inner world and provide an anchor point. For example, a “bear” can represent a powerful, protective knowing or connecting to the word that is on the card “Presence” which is a strength that one will choose to connect to and emphasize. Acknowledging one’s own strengths helps to explicitly identify positive aspects of self and connect with others on positive criteria. There are many different creative decks of cards that can be used for this exercise with different focuses. Group members are invited to share with each other in dyads about why they chose the cards that they chose. This happens at the start of the group and begins the warm-up for participants with a focus on strengths and connection. Sharing in dyads feels much safer for group members than sharing in a larger group. Clients place their OE cards in a visible place around the room where they can be reminded of their strength and the ability to see themselves without judgement. At any point in the group, if a participant becomes dysregulated, the facilitator can use their OE card as a tool for self-regulation. This is often as simple as reminding the client to look at it, stand next to their OE card, or remember why they chose this specific card. If the facilitator has psychodrama training they can instruct the client to reverse roles with their OE and speak to her dysregulated-self from this strength-based role. In this way, the OE role actively works to reverse the negative patterns of self-talk that are so common for survivors of addiction and trauma.
The Circle of Strengths
The identification of strengths is incredibly restorative and healing for persons who have experienced addiction and trauma. Recognizing positive aspects of self helps one in recovery to challenge their negative images of self and renegotiate narratives of self-worth. The Circle of Strengths TSM safety structure, sometimes referred to as The Circle of Safety, is an adaptable action-based group intervention which facilitates an identification of strengths and a deepening of interpersonal connections while providing a visual demonstration of containment (Hudgins & Toscani 2013).
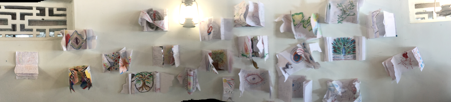
As individuals initially enter into the group space, their curiosity is awoken by a collection of colorful and diverse scarves positioned in the center of the circle of chairs. A facilitator introduces the importance of strengths in the context of the group process and describes the three different categories of strengths: personal, interpersonal, and transpersonal. The personal, or intrapsychic, are strengths that are inclusive to the individual, such as courage, willingness, and intelligence. Interpersonal or relational strengths are qualities that involve others or relationships, examples include: compassion, trustworthiness, a supportive parent, and an important friend. The final category of strengths are transpersonal, or beyond human. For some, this means spiritual or religious, but for others it translates to that which is nonmaterial, for instance: art, music, purpose, and nature.
Historically, the Circle of Strengths began as an acknowledgment of individual strengths during which each group member would choose a scarf to represent a strength that they bring to the group. Many therapists choose to include themselves and their strengths into the circle as they, and their strengths, certainly have a role in the group. Each individual verbally states the strength that their scarf represents and is acknowledged by the group before placing the concretized strengths on the floor in the form of a large circle. For example, “this scarf represents my courage, which helps me to continue improving myself as a person.” The Circle of Strength later evolved culturally through its application in Asia, and was adapted to better compliment a more communal and interpersonal society. Rather than have individual’s identify their own strength, which is experienced as impolite in some cultures, group members are instructed to find a partner and acknowledge a strength that they experience in their partner (Hudgins & Toscani 2013). For instance, “this scarf represents the incredible resilience that I have experienced in you through your story.” The circle of concretized strengths serves as a potent visual reminder for each individual in the group of their own personal resources, as well as the collective power of the group. It can be helpful to invite participants to take a photo, or create a drawing, of the circle of strengths in an effort to offer them another resource for containment or empowerment in between sessions or long after the workshop has ended.
Spectrograms: Group Assessment
A spectrogram is a unique sociometric tool that can be used in the therapeutic process to assess a client and/or group in the “present moment” (Dayton, 2005). Spectrograms are full-scale assessment tools that can be used in the actual clinical environment to measure specific criteria on the group-as-a-whole level. The spectrogram is a life-sized sliding scale from zero to ten in the room. For example, a clinician may be interested in knowing whether her group members are comfortable talking and sharing in a therapeutic group. The clinician can ask participants to picture an imaginary line across the floor connecting to two opposite walls to create a spectrum for the group. One wall could represent the extreme of “I feel extremely comfortable talking and sharing in a therapeutic group,” and the opposite wall could represent “I feel extremely uncomfortable talking and sharing in a therapeutic group.” The clinician would then invite the group members to physically place themselves on the imaginary line, or spectrogram. Once placed on the spectrogram, the clinician can choose to have participants to share with each other or aloud to the group why they placed themselves in their specific location. The clinician now has data from this exercise to better understand some of the group dynamics and the clients in the group will be more familiar with each other’s comfortability within the group.
In Mirmont’s recovery groups the following criteria, guided by TSM’s clinical map, is often utilized. When discussing the different recovery options/programs to maintain sobriety it can be helpful to use spectrograms on discovering the amount of knowledge individuals may have about the 12-step programs, smart recovery, refuge recovery, etc. While on the spectrogram, participants with a large amount of knowledge can be encouraged to share with the group about their own journey as well as have the opportunity to gain further personal insight on what they may have learned. The individuals who have identified themselves as having very little knowledge are given an opportunity to learn from group members about different programs and experiences. The clinician is able to discover the group’s knowledge base on recovery options – with this data the clinician is better able to meet the specific educational needs of the group. Clinicians can also use spectrograms to assess a client and/or group’s comfortability with asking for help, awareness of relapse triggers, degree of healthy coping skills, trauma history, etc. The clinician is able to use this tool to gain data for further treatment as well as promote connection among the members as they learn more about one another and share their present moment states.
It is important to remember that this sociometry tool relies on the client’s self-assessment of where they fit in on the spectrogram. In our experience, clients tend to under-report on positive criteria while over-reporting negative criteria. When choosing positive criteria, it helps start the spectrogram at a positive number instead of zero. For example, with the spectrogram criteria of “how resilient do you judge yourself to be?”, designating one side of the room as ten out of ten in resilience with the other side of the room being five of ten. This provides added containment and prevents group members from under-valuing their strengths. The choice of criteria based on TSM’s clinical map provides a built-in system for warm-up and containment – pendulating into the trauma and back out. This allows group members to work with painful material in short contained segments in between positive criteria.
Action Sociograms
The Action Sociogram, often called Hands-on-Shoulders Sociometry, is a sociometric action method that reflects the healing power of touch and focuses on group members’ experiences of each other. The emphasis on safety has been instrumental in Mirmont’s use of hands-on-shoulder in experiential group work. Practitioners relay the importance of asking permission before placing a hand on the shoulder of another patient which becomes empowering, especially for trauma survivors. In action sociograms, criteria is offered by the facilitator (also following TSM’s clinical map) and participants answer the criteria-based question by placing a hand on the shoulder of one group member. For example, “who do you feel closest to in the group?” “who would you choose to play the role of your strength?” “who would you choose to play the role of your addiction?” or “who’s topic do you most identify with?” Each question results in a new configuration of choices demonstrated in action and concretized by a hand on another’s shoulder. This sociometry tools demonstrates what Moreno describes as the sociodynamics effect – the unequal distribution of social wealth within a group (Moreno, 1953). As group leaders, it is important to be aware of the sociometric stars and isolates within the group and to craft exercises that reverse the sociodynamic effect.
The effectiveness of touch as a tool can be traced back to Moreno’s development of group psychotherapy and psychodrama in the 1930’s where nurses played an integral part in the development and maintenance of the therapeutic community (McIntosh, 1999). Moreno observed and attested to the benefits experienced by patients when a nurse made physical contact by holding a hand or placing a hand on a shoulder to settle a person thereby alleviating their suffering (McIntosh, 1999). More recently, Jakubiak & Feeney (2017) have provided a review of the research on physical touch and its relationship to wellbeing. Touch has sometimes been referred to as a fifth sense because the skin is the oldest and largest of our sense organs and the first to develop (Field, 2011). Moreno incorporated bodily contact as an effective means of providing a patient with a sense of immediate connection to the world and to another human being (McIntosh, 1999). This bodily contact and the healing power of touch can be seen in 12 step communities where groups have incorporated holding hands, locking arms, and hugging as central tenets of demonstrating connectedness.
Action Sociograms are often used to choose group topics or psychodrama protagonists, allowing patients to see their choices displayed in action. Sociograms can also be completed on paper by graphing the social attractions and repulsions between individuals within a group or community – the sociogram is the forerunner of the genogram, ecomap, and social network (J.D. Moreno, 2014). This visual conceptualization and measurement of the social choices has been one of Moreno’s most significant contributions to sociometry (Treadwell et al, 1997).
Step-in Sociometry: Identifying Similarities (Sharon)
Another form of sociometry, and a way of warming up and building group cohesion in early recovery, is Step-in Sociometry (Buchanan, 2016). This tool helps patients connect through their similarities, as opposed to their differences. Often, individuals who are struggling with addiction will be preoccupied with circumstances, believing they cannot relate to someone else’s life story, thus perpetuating isolation. In experiential groups, step-in sociometry creates a foundation for connecting the patient to peers through shared aspects of identity and shared experiences. The Therapeutic Spiral Model’s (TSM) clinical map is used to guide criteria choices – beginning with safety and strengths, then trauma and addiction, ending with meaning making and transformation (Giacomucci, 2017). The process begins with the group standing in a circle and one person making a statement about herself while taking a step into the circle. Other group members who agree or identify with the statement take a step into the circle too. This is a form of non-verbal sharing that allows the group to quickly identify similarities in a non-threatening manner. Participants can take turns making step-in statements, or it can be done spontaneously.
In the following example, we integrated the content of Gorski’s relapse prevention warning signs into action (Gorski, 2016; Gorski & Miller, 1986). The first statement, practicing safety and cohesion, fosters connections based on similarities. “My favorite healthy spare-time activity is…” Peers can identify with one another, which helps patients to ease into knowing their peers. The second statement is moving into the spiral of experiencing the addiction, “one thing I lost through my addiction was…” The next two statements have a double step-in, based on Gorski’s warning signs. These foster a shared experience and connection, by detailing how relapse progression appears for different patients. The double step-in allows sharing both the warning sign and the reaction/feeling. “I know I’m in trouble in my recovery when I… and I…” and “when I’m feeling overwhelmed I… and…” Both of these statements begin as normal step-in criteria, but evolve into a second layer of identification and stepping-in. The final strand of the TSM clinical map is transformation, demonstrated by the final step-in criterion, “I feel hopeful when…” Other step-in sociometry criteria that can be applied in clinical groups include: self-care activities, defense mechanisms, future goals, or favorite aspects of recovery. By the end of the exercise, the group is aware of the similarities and shared experiences that they have. Step-in sociometry allows the group to uncover the previously invisible similarities that connect group members.
Conclusion
While many addiction and trauma group approaches focus on client similarities in their experience of addiction and trauma, sociometry guided by TSM’s clinical map has the power to provide experiences of connection based on positive criteria. Instead of trading addiction war-stories, clients trade strengths and hopes. Many inpatient clients feel as though they are ostracized from their families and communities, and the last place they would expect to experience a welcoming community is in an inpatient addiction treatment center. We argue that an inpatient unit is uniquely positioned to provide this type of corrective emotional, relational, and communal experience. Many drug users indicated that they only feel a sense of belonging when they are with others who also use drugs, so to this effect, an authentic sense of belonging without drugs is incredibly restorative. Clients often enter treatment in a state of psychosocial dislocation; sociometry can provide an experience of psychosocial integration and an enhanced sense of belonging (Hale, 2009). Interpersonal Neurobiology research shows that new experiences change the brain (Cozolino, 2014; Siegel, 2012; van der Kolk, 2014); sociometry and psychodrama have the power to access this corrective potential. While many group approaches can be better described as treating an individual within a group setting, sociometry is treating the group-as-a-whole.
References
Alexander, B.K. (2008). The Globalization Of Addiction: A Study In Poverty Of The Spirit. New York, NY: Oxford University Press.
Buchanan, D.R. (2016). Practical Applications of Step-In Sociometry: Increasing Sociometric Intelligence via Self-Disclosure and Connection. Journal of Psychodrama, Sociometry, and Group Psychotherapy, 64, 71-78
Cozolino, L. J. (2014). The Neuroscience of Human Relationships, (2nd Ed). New York: W.W. Norton & Company.
Courtois, C. A. & Ford, J. D. (2015). Treatment of Complex Trauma: A Sequenced, Relationship-Based Approach. New York, NY: The Guildford Press.
Dayton, T. (2005). The Living Stage: A step-by-step guide to psychodrama, sociometry, and experiential group therapy. Deerfield, FL: Health Communications Inc.
Dayton, T. (2014). Relational Trauma Repair (RTR) Therapist’s Guide, Revised Edition. New York, NY: Innerlook, Inc.
Dayton, T. (2015). NeuroPsychodrama in the Treatment of Relational Trauma: A Strength-based, Experiential Model for Healing PTSD. Deerfield Beach, FL: Health Communications, Inc.
Eisenberger, N.I. (2012). The neural bases of social pain: Evidence for shared representations with physical pain. Journal of Psychosomatic Medicine, 74(2): 126–135.
Erikson, E. (1963). Childhood and society. New York: W.W. Norton & Company.
Field, T. (2011). Touch for socioemotional and physical well-being: A review, Developmental Review, 30, 367-383
Flores, P.J. (2011). Addiction as an Attachment Disorder. New York, NY: Jason Aronson, Inc.
Fuhlrodt, R.L. (ed)(1990). Psychodrama: It’s Application to ACOA and Substance Abuse Treatment. East Rutherford, NJ: Thomas W. Perrin Inc.
Giacomucci, S. (2017). The Sociodrama of Life or Death: Young Adults and Addiction Treatment. Journal of Psychodrama, Sociometry, and Group Psychotherapy 65(1): 137-143
Giacomucci, S. (in-press). The Trauma Survivors Inner Role Atom: A Clinical Map for Post-Traumatic Growth. Journal of Psychodrama, Sociometry, and Group Psychotherapy.
Gorski, T.T. (2016). How to Start Relapse Prevention Support Groups. Self-Published: Bookbaby.
Gorski, T. T., & Miller, M. (1986). Staying sober: A guide for relapse prevention. Independence, MO: Independence Press.
Hale, A.E. (1981). Conducting Clinical Sociometric Explorations: A Manual for Psychodramatists and Sociometrists. Roanoke, VA: Royal Publishing Company.
Hale, A.E. (2009). Moreno’s Sociometry: Exploring Interpersonal Connection. Group, 33(4): 347-358.
Herman, J. L. (2015). Trauma and Recovery: The Aftermath of Violence–From Domestic Abuse to Political Terror. New York, NY: BasicBooks.
Hudgins, M.K. (2017) PTSD Unites the World: Prevention, Intervention and Training in The Therapeutic Spiral Model. In C.E. Stout and G. Want (eds). Why Global Health Matters: Guidebook for Innovation and Inspiration. Self-Published Online.
Hudgins, M.K. & Toscani, F. (2013). Healing World Trauma with the Therapeutic Spiral Model: Stories from the Frontlines. London: Jessica Kingsley Publishers.
Jakubiak, B.K. & Feeney, B.C. (2017). Affectionate Touch to Promote Relational, Psychological, and Physical Well-Being in Adulthood: A Theoretical Model and Review of the Research. Personality and Social Psychology Review, 21(3) 228–252
Jellinek, E.M. (1952). Phases of Alcohol Addiction. Quarterly Journal of Studies on Alcohol, 13(4), 673–684
Lawrence, C. (2015). The Caring Observer: Creating Self-Compassion Through Psychodrama. The Journal of Psychodrama, Sociometry, and Group Psychotherapy 63(1): 65-72
Maté, G. (2010). In the Realm of Hungry Ghosts: Close Encounters with Addiction. Berkeley, CA: North Atlantic Books.
McGregor, I.S. and Bowen, M.T. (2012). Breaking the loop: Oxytocin as a potential treatment for drug addiction. Hormones and Behavior, 61(3): 331-339
McIntosh, W.H. (1999). A Critical History of the Influence of Jacob. L. Moreno’s Concepts and Techniques on Nursing 1930s-1990s. Unpublished Master’s Thesis, Queensland University of Technology, Brisbane, Australia.
Moreno, J.D. (2014). Impromptu Man: J.L. Moreno and the Origins of Psychodrama, Encounter Culture, and the Social Network. New York, NY: Bellevue Literary Press.
Moreno, J.L. (1937). Sociometry in relation to other social sciences. Sociometry, 1: 206-219
Moreno, J. L. (1953). Who Shall Survive? Foundations of Sociometry, Group Psychotherapy and Sociodrama (2nd edition). Beacon, NY: Beacon House.
Panksepp, J., Herman, B., Conner, R., Bishop, P., & Scott, J. P. (1978). The Biology of Social Attachments: Opiates Alleviate Separation Distress. Biological Psychiatry, 13(5), 607-618.
Porges, S. W. (2017). The Pocket Guide to The Polyvagal Theory: The Transformative Power of Feeling Safe. New York, NY: W.W. Norton & Company
Siegel, D.J. (2012). Developing Mind: How Relationships and the Brain Interact to Shape Who We Are. New York: Guilford Press.
Substance Abuse and Mental Health Services Administration (SAMSHA) (2017). Focus on Prevention. HHS Publication No. (SMA) 10–4120. Rockville, MD: Center for Substance Abuse Prevention, Substance Abuse and Mental Health Services Administration.
Tierney, M. (1945). Psychodramatic Therapy for the Alcoholic. Sociometry, 8(1): 76-78.
Treadwill, T.W., Kumar, V.K., Stein, S.A., Prosnick, K. (1997). Sociometry: Tools for Research and Practice, Journal for Specialists in Group Work, 22(1): 52-65
Van der Kolk, B. A. (2014). The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma. New York: Viking Press.